What is Pellucid Marginal Corneal Degeneration (PMD)? In short it is an eye disease very similar to Keratoconus in that it also causes thinning of the corneas. The difference between Keratoconus and Pellucid Marginal Corneal Degeneration is that PMD causes a crescent shaped band of thinning in the lower region of the eye, while the central cornea is usually of a normal thickness; as well as the cornea appearing transparent in PMD . There is a third disease called Keratoglobus that like the previous two also causes corneal thinning (more about this disease will be discussed in a future post).
Now you may ask if there is an actual difference between Keratoconus and PMD and Keratoglobus or if the three diseases are the same. The answer is that doctors are not sure either. They do not know if the three eye diseases are different diseases, or just different phenotypic (expression) variations of one disease.
Some of the different signs of PMD may include drastically reduced uncorrected visual acuity that usually cannot be improved with glasses (usually for astigmatism), roughly normal pinhole visual acuity, and refraction/keratometry that shows against the rule astigmatism (where the astigmatism on a corneal topography is seen horizontally).
Patients are also commonly asymptomatic except for the gradual worsening of vision that is unaided by glasses. The clinical diagnosis for PMD is the same as Keratoconus where the patient is examined by doctor on a slit lamp microscope and checked with patient’s history and supported by corneal topography & pachymetry.
We have been talking about how cross linking can help patients suffering from Keratoconus. We may’ve a bigger issue to confront. What about before cross linking, what about the diagnosis and screening of Keratoconus. It is important for patients with Keratoconus to be screened as early as possible. The best results with corneal cross linking eye procedure are obtained when the disorder is arrested early. As the disease progresses the loss of visual acuity increases dramatically, and the earlier it is detected the easier and higher possibility that full visual acuity returns. You may want to read some frequently asked questions on keratoconus and cross linking.
Some symptoms of Keratoconus are blurry vision, increased light sensitivity, eye strain, headaches/general eye pain, eye irritation/excessive eye rubbing. A caution should be noted that these symptoms can also be indications of other eye problems. That is why it i important to see a keratoconus expert. The doc in conjunction with measurement of the curvature of the cornea, a depth map and examining the eyes can identify the disease more early and accurately.
From a doctor’s perspective, as they physically examine the eye with a microscope, the signs they would be looking for are corneal thinning, Fleischer’s ring, Vogt’s striae, and apical scarring. The measuring of the corneal curvature can be done three different ways: first would be keratometry, second is corneal tomography, and third is a corneal OCT. Though all three should performed for increasing the accuracy of the measurement.
Now that you have a basic understanding of importance of early detection try our quiz on keratoconus.
We talked last time about getting screened for Keratoconus and the importance of early diagnosis. Today let’s talk about what to expect after the cross linking procedure has finished. Immediately after the UV-A light part of the surgery is over, a bandage contact lens will be put in the eye. This is done in order to protect the eye from dust,wind, et cetera. The second important reason is that it prevents the lid from rubbing the abraded cornea. If it is not put or falls off the lid like a windshield wiper can sweep healing cells and irritate the corneal nerves. A topical antibiotic, a non-steroidal anti-inflammatory (NSAID), 4 times a day for the first week.
A steroid will be prescribed once the epithelium has healed completely.The steroid being usually continued for another 1-3 weeks.
The Keratoconus surgeon will usually follow up with an appointment with in 24 to 48 hours as well as the week following surgery to make sure the eye is healing properly. If needed, after the epithelium is intact, the doctor would send the patient’s back to co-managing doctors for the remainder of their follow up care.
We all have to be careful during the post period to avoid touching or rubbing the eye. Some discomfort and watering of the eye is to be expected. If you develop sever pain or discharge contact doc immidiately.
New Scleral contacts or old soft lens may continued under the watchful eyes of the keratoconus doctor.
I am amazed when doctors claim that they have invented a procedure even though it has existed for years before. For example a surgeon claiming they invented cornea cross linking even though it was being performed in Europe for many years.
What gets me peeved is that some doctors use unproven technology and convince patients its the best. Snake oil sellers are an amusement till patients are harmed. So I decided to list some truths about keratoconous eye disease and cornea collagen cross linking.
The 10 Golden Truths about Cornea Cross Linking By Rajesh Khanna, MD a Keratoconus specialist.
Keratoconus is a sight threatening disease. It involves the thinning and bulging of the cornea.
Recent data suggests it may be more prevalent than 1 in 2000 people
Cornea Collagen Cross Linking (CXL) is a proven and effective way to halt the progression of progressive keratoconus eye disease.
CXL may be used to stabilize post lasik ectasia.
Epithelium off Cornea cross linking is more effective than epi on cross linking.
Conventional cornea cross linking – 3 mw for 30 minutes is the gold standard.
Conventional cross linking is more effective than accelerated cross linking (18 mw or 30 mw). No other power setting is better.
No studies have shown epi on cross linking to be more effective than conventional epi off cross linking.
FDA has only approved Avedro KXL system/Photrexa for treatment of progressive keratoconus. No other system nor riboflavin compound has passed that litmus test.
Avedro KXL/ Photrexa which treats at 3mw is currently safer and more effective than other currently available epi on choices in Los Angeles
I would invite comments by optometrists, ophthalmologists and peers especially keratoeonus experts.
Avedro KXL system in the hands of an experienced Keratoconus surgeon following FDA protocols would be safer than an unproven experimental epi on technology. We therefore offer Avedro cornea collagen cross linking with the FDA approved protocol.
We have been receiving a lot of questions from patients via social media and telephone calls. People out there are confused regarding the safety and efficacy of the various advertised treatment methods for keratoconus. This is a quick recap of the currently available interventions to help people suffering from keratoconus eye disease. We have Intacs, Cornea Cross Linking, DALK and Corneal transplant. DALK and Corneal Transplant are surgical techniques and thus are not in the purview of the FDA. Let us confine our discussion today than to Intacs and Cross Linking for keratoconus eye disease.
Intacs for Keratoconus are FDA approved
Yes Intacs are the only intracorneal ring implants approved by FDA. Others like Ferras rings are not approved and cannot be sold in USA. Dr. Khanna is one of the participants in an Institutional Review Board monitoring by Integrview. This ongoing oversight ensures that the results are safe.
Is Corneal Cross linking FDA approved?
There are three types of Corneal cross linking available in the US today.
FDA approved : There is one and only one FDA approved – KXL device and riboflavin called Photrexa manufactured by Avedro. This means that Avedro did a clinical study to demonstrate the safety and efficacy of their formulation with their unique device. Data was submitted to the FDA. Federal Drug and Administration studied the reports. They asked questions and requested more data. Once this was reviewed FDA approved the Avedro method.
Clinical studies : There are clinical studies being performed by different groups like the AECOS and CXL study groups. FDA has not given the green light on them.
God Given: These are devices which doctors cannot explain how they arrived in their offices or surgery rooms. The data from these unexplained devices is not being submitted to FDA nor even peer review. No one knows what drugs are being used.
Which one should you use?
FDA ensures the safety of our eyes. They review the statistical data to keep us safe. Therefore when comparing different treatments it is easier for us to know which is safer.
Since there is only one FDA approved cross linking procedure, choose AVEDRO Cornea Cross Linking.
Learn more about treatment modalities for keratoconus.
We have been talking about the advantages of epithelium off cross linking. This from of cross linking has shown to work in numerous studies across the world.
But are all delivery methods the same? Certain machines hope the patient keeps looking at the UV light. Have you tried staring at something for 30 minutes. As a kid you may have played the stare off game. Its tough to do it especially in Los Angeles with the dry weather.
The solution in this fight against keratoconus is to involve a pupil tracker. In the above video you will see it in action. If the eye moves away from the light, the UV delivery and timer will stop. You can set how much movement you are willing to allow.
This increases the safety. One can definitely know that 30 minutes was delivered. It can avoid a situation where a fidgety patients moves and receives only 20 minutes of the radiation. Increasing safety also relaxes the patients. Most of the people requiring this intervention against Keratoconus eye disease are teenagers. Pupil tracking rocks.
Epithelium off Cornea collagen cross linking (CXL) is not voodoo. We realize that early in new technology a lot of unfounded claims like epi on CXL being Better than epi off might be made. It behooves us clinicians to present proof to peers.
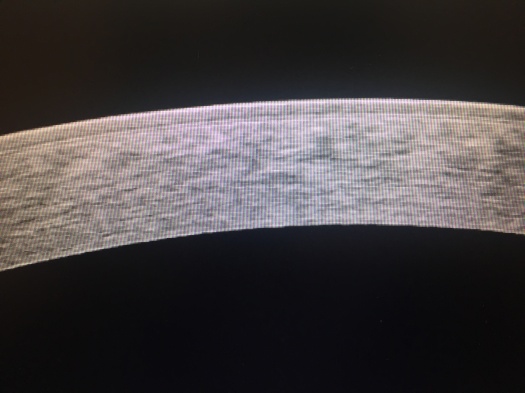
There is a symbiosis between diagnostic technology and treatments. We will take help of Carl Zeiss Ocular coherence tomography to demonstrate the effectiveness of epi off CXL.
Here is a High Density picture of a keratoconus cornea before any treatment. It is early keratoconus in a young girl. This is the best time to intervene to treat Keratoconus. Look how uniform the picture is. The top layer of epithelium can be clearly seen. We remove this layer with laser or as Professor Theo Seiler recommends with ethyl alcohol.
Epithelium prevents riboflavin from entering the stroma and hinders the UV absorption. Look at the picture below. You can clearly see a haze which ends around 80 % depth as a line of demarcation.
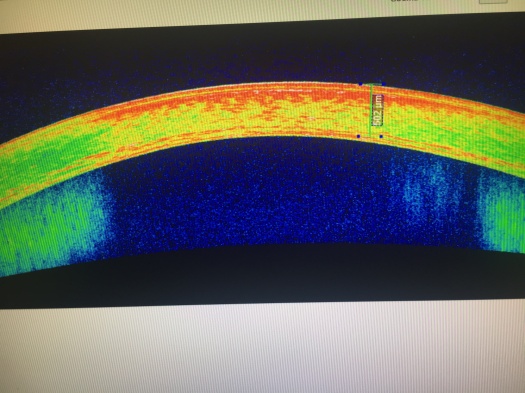
The same line of demarcation after cornea cross linking is better highlighted in they colored OCT of the Cornea.
If you are suffering from Keratoconus Call 805-283-6520 to see if cross linking of cornea is the best option for you.
We pose this question as many medical insurances deny patients reimbursement for cornea cross linking to treat keratoconus. Many parents also pose this question as their own optometrists were unaware of the benefits of cross linking the cornea.
We are going to turn to Australia for a peer review objective answer to this question. Our Australian colleagues performed a study which has been vetted by our peers. The Australian keratoconus experts selected 100 eyes with progressive keratoconus eye disease. They divided them into 2 groups. One would receive Conventional cornea cross linking while the other would have no intervention ( like your insurance company would want). They measured various data like vision, cornea thickness, and curvature of the cornea at various intervals over a period of 3 years.
Are you ready for the results? Can you guess what they showed?
Yes Conventional Cross Linking with UV-A applied on riboflavin soaked eyes was able to prevent steepening of the cornea. It preserved vision both uncorrected and best corrected. It also improved the shape and vision in many instances. We are so convinced by the results we would not be able to repeat it here in the United States. For we would not condemn any kid with keratoconus to be in the control group. The benefits are so obvious. Like society eradicated Polio it is time to wipe away keratoconus eye disease.
Feel Free to print the abstract from the respected Journal Ophthalmology which is attached as an image to show your doubting doc, illogical insurance rep or obstinate optometrist.
BMW on the autobahn is a hair rising experience. Now our German friends want to bring that concept to cxl or corneal cross linking. You may have heard of accelerated cornea cross linking? This is cxl with 10 minutes of UV radiation treatment, In the newest version they propose treatment of only 5 minutes utilizing 18 mw/cm2 of UV radiation.
This would of great benefit to patients. The amount of time they have to stare at the blue light would decrease. Exposure of the cornea to the elements would be less.
We would like to quote the results of the study here ” The mean follow-up time was 21.7 ± 7.2 months (range, 12-34 months). No statistically significant changes were found in the mean corrected distance visual acuity, corneal astigmatism, Kmean, Kflat, Ksteep, corneal pachymetry (at the apex and at the thinnest point), and corneal densitometry at follow-up. A significant reduction of Kmax, index of surface variance, index of vertical asymmetry, and Km of the posterior corneal surface (Km(B)) was observed (Kmax: P = 0.018; index of surface variance: P = 0.016; index of vertical asymmetry: P = 0.038; Km(B): P = 0.008). No complications were reported during the postoperative follow-up period in this study.”
Our question for the authors are. 1) How deep was the demarcation line?
2) was any comparison made to conventional cross linking?
Other papers or followup studies should be address the questions.
Dr.Khanna is a Keratoconus Expert. These informative blog posts are for information purposes. They should not replace a careful discussion with you Keratoconus Eye surgeon.
Keratoconus eye disease is no laughing matter. It afflicts teens and can destroy careers. We need to accelerate our fight against this vicious disease. At the same time we have to study scientifically the newer protocols. Accelerated cross linking speeds the treatment by decreasing the time of exposure of UV light. This has recently been studied in pediatric keratoconus.
This landmark study from Hong Kong By Surgeons of Royal college is a landmark one. It shows that accelerated cornea cross linking slows the progress of the bulging eye disease. it is the first one to document that only conventional cornea cross linking with its deep demarcation line can actually flatten the cornea. In essence it means that the 30 min api off intervention can halt the progression as well as reverse some of the effects.
The deeper the demarcation line the more the cornea flattening .
Keratoconus Experts in Los Angles thank the authors to bring new meaningful data for mutual benefit.
Update terbaru menghadirkan map baru yang luas, lanjut ke ulasan Keluaran macau. Update terbaru memperbaiki sistem matchmaking. Pertandingan jadi terasa lebih seimbang.
Slot Gacor Online menawarkan berbagai variasi permainan yang cocok untuk semua jenis pemain. Mulai dari yang suka permainan cepat hingga yang menikmati strategi, semuanya tersedia di sini.
Kombinasi simbol dalam permainan ini sangat menentukan keberhasilan pemain dalam meraih kemenangan besar. Pemahaman terhadap mekanisme permainan akan sangat membantu dalam menciptakan strategi yang lebih efektif. Tidak heran jika semakin banyak orang yang tertarik untuk memainkan Mahjong Ways 2.
Promo top-up ini sangat cocok untuk kamu yang ingin mendapatkan resource lebih banyak dengan harga lebih hemat lihat informasinya pedetogel link alternatif. Tips leveling cepat bisa dilakukan dengan konsisten menyelesaikan misi harian. Cara ini terbukti cukup efektif.
Cara cepat naik tier tanpa harus main nonstop ternyata ada triknya sendiri, tutorial lengkap di bd-innovations.com. Banyak pemain mencari setting grafis terbaik untuk FPS stabil. Performa lancar memang penting saat pertandingan kompetitif.
Event mini game dalam game utama ini ternyata kasih reward utama kalau target tercapai, cara mainnya dijelaskan pada toto. Tips farming efektif adalah pilih map dengan respawn cepat. Efisiensi waktu sangat berpengaruh.
Deposit Kecil Membawa Pengalaman Bermain Slot Tanpa Mengeluarkan Dana Besar
Bermain slot online menjadi lebih hemat dengan adanya Slot Depo 5k. Bagi pemain baru yang masih ingin mencoba-coba, deposit kecil ini memungkinkan mereka untuk merasakan pengalaman bermain tanpa harus mengeluarkan dana besar. Selain itu, fleksibilitas dalam deposit memberikan pemain lebih banyak opsi. Slot Depo 5k benar-benar membawa suasana bermain slot yang ramah di kantong.
Promo top-up hari ini cocok buat stok resource jangka panjang tanpa harus nunggu event besar di toto. Update visual lingkungan bikin map terasa lebih hidup. Detail kecil bikin betah.
Event terbatas ini jadi momen terbaik buat farming item langka dalam Toto. Event komunitas sering menghadirkan hadiah kecil tapi menarik. Partisipasi pemain membuat suasana semakin meriah.
Bukan rahasia lagi, kalau rtp live jadi alat wajib para pemain slot buat nyari slot rtp tertinggi yang paling gacor. Dengan info ini, kamu nggak cuma asal main, tapi bisa pilih slot gacor hari ini yang beneran ngasih peluang besar. Sensasinya beda banget dibanding main asal nebak, tiap spin jadi lebih berarti dan bikin kamu nggak sabar buat putaran berikutnya.
Jika kamu ingin mencoba peruntungan tanpa beban besar, pilihan terbaik adalah Slot 10k yang memberikan kesempatan bermain lebih lama dengan dana yang minim.
Bermain dengan nyaman dan lancar kini menjadi lebih mudah ketika memilih slot server Thailand sebagai pilihan utama, karena kecepatan dan kestabilannya memastikan pengalaman bermain yang menyenangkan tanpa gangguan yang mengurangi fokus dalam meraih kemenangan besar.
Live Draw Macau Transparan Memberikan Kepercayaan Penuh
Melihat angka keluar secara langsung melalui Live draw macau menghadirkan kepercayaan penuh, karena pemain bisa menyaksikan sendiri proses pengundian yang berlangsung terbuka.
Saat fokus mencari kenyamanan dan keamanan, para pemain mengandalkan Situs Togel yang menyediakan berbagai pasaran lengkap, transaksi cepat dan aman, serta informasi angka keluar terbaru yang membantu mereka merencanakan strategi bermain lebih efektif.
Banyak penggemar judi online memastikan taruhan mereka ditempatkan di Togel Resmi yang diawasi secara ketat agar semua hasil angka keluaran valid, transaksi aman, dan hadiah dibayarkan tepat waktu.
Promo top-up dengan bonus item langka ini cuma tersedia hari ini, ketentuannya dijelaskan pada togel. Update fitur sosial bikin interaksi antar pemain makin gampang. Mulai dari chat sampai party system.
Promo top-up terbatas ini ideal buat persiapan turnamen di situs toto. Event spesial weekend biasanya lebih santai. Cocok buat main bareng teman.
Leveling cepat buat karakter kedua bisa lebih gampang dengan metode situs toto. Komunitas biasanya punya istilah sendiri. Pemain baru perlu waktu buat ngerti.
Promo top-up plus voucher lagi dibuka, klaim bonusnya lewat Togel. Update ranking system kadang bikin progress terasa lebih berat. Tetap konsisten, lama-lama naik juga.
Patch baru bawa item yang bikin farming makin cepat, tapi banyak yang belum tau cara pakainya, cek di toto. Event seasonal bikin suasana game berubah total. Map dan musiknya biasanya beda dari biasanya.
Promo top-up ini kasih bonus diamond tambahan kalau beli di jam tertentu, jamnya ada di togel. Event battle pass itu paling efektif kalau kamu konsisten. Sedikit tiap hari lebih ringan daripada kebut di akhir.
Penjelasan Guru Sosiologi Tentang Peluang Hidup
Seorang guru sosiologi menjelaskan contoh perilaku sosial kepada muridnya, lalu di tengah penjelasan ia menyinggung Togel hanya sebagai ilustrasi tentang cara manusia memahami peluang dan harapan.
Turnamen guild yang paling ditunggu pemain akhirnya segera dimulai, jadwal pertandingannya bisa kamu cek pada Togel Online. Event spesial kadang memberikan bonus exp yang besar. Hal ini membantu pemain naik level lebih cepat.
Dengan layanan pelanggan yang siap 24 jam, Situs Togel178 memastikan bahwa setiap pertanyaan dan masalah pemain dapat diatasi dengan cepat dan efektif, memberikan pengalaman bermain yang lebih nyaman.
Dengan layanan pelanggan yang siap 24 jam, Togel178 memastikan bahwa setiap pertanyaan dan masalah pemain dapat diatasi dengan cepat dan efektif, memberikan pengalaman bermain yang lebih nyaman dan bebas dari masalah.
Promo bonus top-up terbatas malam ini bikin player ramai masuk, lengkapnya tautan arah pedetogel alternatif. Patch baru kadang buff karakter lama yang sempat dilupakan pemain. Itu bikin variasi pilihan makin luas.
Tips push exp dan resource sekaligus mulai dicoba, tutorial arah rujukan hk pools 20. Event double drop selalu jadi waktu favorit buat grinding. Hasil farming biasanya jauh lebih maksimal saat itu.
Partner Links
Petaruh www.resea-rchgate.net Singapore mengandalkan data lengkap SGP untuk pasang angka jitu mereka.
Para pemain toto di sini Rtp Togel178 takkan suntuk, beragam pasaran togel siap dimainkan.
Bonus deposit Togel 279 sangat menguntungkan bagi pemain poker online.
Cara Togel158 bermain yang fleksibel membantu pemain bergabung ke situs judi terpercaya.
Kami siapkan analisis tenis lengkap dengan statistik Togel158 pertandingan, rekor head-to-head, dan performa terkini.
Cara termudah untuk menerapkan Togel178 spekulasi hebat ini agar pemain merasakan servis yang lebih baik.
Situs ini tidak cuma tempat bermain, tapi juga sumber panduan bermanfaat dan macauindo.co mendalam.
Strategi tidak selalu https://pedetogel.net/ sempurna, tetapi dengan latihan terus, keterampilanmu akan tajam.
Di sini, kami akan bagikan panduan sukses menang Togel178 dalam permainan Kompetisi online terbaik.
Ini telah jadi faktor utama Situs Pedetogel Rekreasi online sukses sampai sekarang.
Registrasi simpel dan cepat, dimulai main sabung https://kampuspoker.com/ ayam online dengan cepat.
Akhirnya, kami situs togel ingin menegaskan pentingnya sabar dan disiplin dalam bermain Aktivitas Seru secara daring.
Dengan cara ini, Slot Gacor Anda bisa tingkatkan keuntungan dan sukses dalam perjudian.
Berkumpul dengan teman di tempat nongkrong bisa kaya situs idn poker lewat permainan 1 tanpa bekerja.
Banyak pemain togel memilih Colok178 sebagai situs andalan mereka. Selain memiliki reputasi terpercaya, Colok178 menawarkan kemudahan transaksi melalui berbagai metode, termasuk e-wallet dan bank lokal. Dengan peluang menang yang tinggi, situs ini menjadi favorit banyak kalangan pencinta togel.
Banyak bettor mencari situs yang tidak hanya aman tetapi juga memberikan banyak keuntungan tambahan. Pedetogel menawarkan berbagai promo menarik yang dapat meningkatkan peluang kemenangan pemain. Dari bonus deposit hingga cashback, semuanya tersedia bagi para pengguna setia. Selain itu, situs ini memiliki sistem transaksi yang sangat cepat dan fleksibel, memungkinkan pemain untuk menikmati permainan tanpa hambatan. Dengan berbagai keunggulan ini, tidak heran jika situs ini semakin diminati.
Bagi pemain yang ingin mendapatkan hasil terbaik, situs macau menawarkan berbagai pilihan bonus dan promosi yang terus diperbarui. Pemain bisa memanfaatkan kesempatan ini untuk meningkatkan peluang menang mereka di setiap taruhan.
Bermain togel online bukan hanya soal keberuntungan tetapi juga soal memilih platform yang terpercaya. Salah satu cara memastikan keamanan bermain adalah dengan bergabung di situs togel resmi yang memiliki reputasi baik. Situs ini menggunakan sistem keamanan tinggi dan pembayaran yang cepat untuk menjamin kenyamanan pemain. Selain itu, berbagai fitur tambahan seperti statistik angka dan analisis tren juga disediakan untuk membantu pemain meningkatkan peluang menang.
Salah satu fitur menarik yang kini populer di kalangan pemain adalah cashback mingguan. Bonus ini memungkinkan pengguna untuk mendapatkan kembali sebagian dari kekalahan mereka. Tidak heran jika Toto92 menjadi favorit karena rutin memberikan cashback dan promosi lainnya.
Dalam memilih situs permainan online, penting untuk memperhatikan reputasi serta pengalaman yang dimiliki oleh platform tersebut. Toto92 sudah lama dikenal sebagai salah satu pionir dalam industri ini. Dengan pengalaman bertahun-tahun, mereka paham apa yang dibutuhkan pemain dan selalu berupaya memberikan yang terbaik. Hal ini menjadi alasan utama banyak pemain tetap setia.
Salah satu hal yang membuat platform hiburan digital berkembang pesat adalah kepercayaan pengguna. Nama Sabatoto muncul sebagai pilihan yang konsisten menjaga kualitas dan memberikan pelayanan terbaik. Hal ini dibuktikan dari banyaknya ulasan positif yang beredar.
Platform yang ramah pengguna biasanya mendapat tempat di hati masyarakat. Hal inilah yang menjadi fokus dari Pedetogel, menciptakan pengalaman tanpa ribet untuk semua kalangan.
Menjadi bagian dari komunitas Togel178 memberikan keuntungan tersendiri karena ada banyak tips dan strategi dari para pemain senior.
Karena sering kesulitan klaim bonus di situs lain, saya akhirnya pindah ke Pedetogel dan ternyata di sini semua promosi bisa diklaim otomatis tanpa perlu menghubungi admin atau repot isi form.
Layanan aplikasi mobile yang disediakan oleh Togel158 membuat pengalaman bertaruh semakin fleksibel dan praktis, karena pemain bisa mengakses permainan kapan pun dan di mana pun tanpa batasan perangkat.
Tidak hanya mengutamakan kecepatan transaksi, Sabatoto juga menjamin semua pasaran yang tersedia adalah resmi dengan hasil angka yang selalu transparan dan akurat.
Sistem notifikasi otomatis di Togel178 memberi info update cepat sehingga di tengah jadwal padat, pemain tidak ketinggalan hasil draw atau promo terbaru dari situs.
Dalam urusan pembayaran, Togel178 selalu memproses penarikan dengan cepat sehingga pemain tidak perlu menunggu lama untuk menikmati hasil kemenangan mereka.
Deposit melalui e-wallet, pulsa, maupun transfer bank bisa dilakukan dengan mudah di Pedetogel sehingga pemain memiliki banyak pilihan transaksi sesuai kebutuhan.
Pemain yang aktif setiap hari berkesempatan mendapatkan reward tambahan dari Pedetogel melalui program loyalitas khusus.
Bagi para pemain lama, Sabatoto menjadi tempat favorit karena selain lengkap, mereka juga konsisten membayar kemenangan tepat waktu.
Banyak promo cashback dihadirkan oleh Sabatoto sebagai bentuk apresiasi untuk para member setia yang terus bermain dan menikmati setiap pasaran yang tersedia.
Bagi yang baru ingin mencoba judi togel online, Togel279 menyediakan panduan lengkap yang membantu pemula memahami cara taruhan hingga teknik prediksi angka dengan mudah.
Para penggemar togel sangat puas dengan layanan dari Togel279 yang selalu memberikan update angka keluaran secara real-time, sehingga tidak perlu menunggu lama untuk mengecek hasil.
Semua pemain yang bergabung di Togel158 dapat menikmati fasilitas discount dan bonus yang membuat setiap taruhan jadi lebih hemat dan berpeluang meraih kemenangan besar.
Togel158 memastikan setiap proses pendaftaran member baru berjalan cepat dan tanpa kendala, sehingga siapapun dapat langsung menikmati berbagai layanan unggulan yang tersedia di platform ini.
Tidak hanya itu, Colok178 juga menawarkan berbagai fitur tambahan yang dirancang khusus untuk meningkatkan kenyamanan pengguna dan mendukung permainan yang lebih seru.
Banyak orang memilih untuk bermain di Togel279 karena reputasinya yang terpercaya serta dukungan layanan yang responsif setiap saat tanpa henti.
Banyak bettor yang menilai keberhasilan mereka dalam taruhan meningkat setelah menggunakan berbagai tools analitik dan statistik pertandingan yang disediakan secara lengkap di Sbobet88.
Bagi mereka yang sudah berpengalaman, bermain dengan slot bet 200 memungkinkan eksplorasi bonus besar dan fitur premium, memberikan rasa puas yang berbeda dibanding taruhan minimal.
Proses pendaftaran di agen permainan resmi sangat sederhana karena alurnya sudah dioptimalkan melalui dukungan Pedetogel sehingga pemain dapat bergabung cepat.
Proses pendaftaran pada agen resmi berjalan lancar dibantu integrasi Togel279 yang membuat seluruh tahapan lebih mudah dipahami.
Proses pendaftaran pada agen hiburan angka resmi yang terhubung Togel Resmi dibuat sederhana agar mudah diakses semua kalangan.
Proses pendaftaran pada layanan resmi dibuat praktis karena Bandar Togel mengutamakan efisiensi tanpa mengurangi keamanan akun.